By: Julian Xie, MD, MPP with contributions from Carolyn Vega, Ceci Henriquez, and Kelleen Zubick from the Share Our Strength team
In this post, we summarize what we’ve been tracking in the federal Medicaid and food security landscape, discuss some brief history of the first Trump Administration’s approach to HRSN (health-related social needs, used almost interchangeably with social drivers of health (SDOH)), and look forward at how we as a network may continue advancing food and nutrition security for children and families through Medicaid policy. Despite much dialogue surrounding Medicaid and SNAP since Trump’s inauguration, it’s still too early to know what’s truly ahead, and we’ll continue to monitor developments and provide updates plus calls to action to the Medicaid Food Security Network.
- Medicaid, SNAP, and WIC are critical federal programs that improve health, and food and nutrition security. Cuts to any one of these programs threatens the other because these programs are mutually-reinforcing and interconnected both at the participant level, and at the agency level when it comes to data-sharing and organizational efficiencies.
- Two calls to action: contact your member of Congress to protect SNAP to support the food and nutrition security of children and their families, and contact members of Congress to protect Medicaid.
- MFSN will continue to support Medicaid strategies for food security. These strategies remain on the table, though the field may shift away from 1115 waivers and towards other Medicaid policy tools and existing flexibilities.
- The previous Trump administration supported efforts to address social drivers of health/health-related social needs (SDOH or HRSN) in Medicaid, and RFK Jr. is supportive of Food is Medicine. We don’t yet know how HHS’s ambitious agenda interacts with the cuts proposed across health and nutrition benefits. Either way, FIM is a potential common ground through which we can advance our shared mission of mobilizing the Medicaid system to support food and nutrition security.
Medicaid, SNAP, and WIC – it’s all connected
Congress is considering numerous options to reduce Medicaid and SNAP spending to pay for tax cuts that would mostly benefit wealthy people. As part of the Budget Reconciliation process, the House Budget Committee has passed a budget resolution that proposes $880 billion in spending cuts to programs under the Energy & Commerce Committee and $230 billion in cuts that will likely come out of SNAP. Most of the cuts would likely come from Medicaid because the Trump administration has stated it won’t cut Medicare. While Budget Reconciliation avoids the 60 Senate votes needed to prevent a filibuster and instead only requires a 50 Senator majority, it’s a multi-step process that will require near-unanimity from House and Senate Republicans to pass.
The Senate’s budget resolution takes a different approach, focusing on defense, energy, and border policy. While the Senate strategy leaves most of the health focus for a potential second reconciliation process later this year, some Medicaid cuts could still be included in the first package. It remains unclear how House and Senate Republican leadership plan to resolve their competing approaches over the coming weeks. While it’s critical to talk about what’s going on and proactively communicate with our legislators, it’s also important to remember everything we’re talking about is only a proposal at this time.
This would be achieved through some combination of per-capita spending limits, work-reporting requirements (which could put an estimated 36 million people at risk to lose coverage), and reductions in Federal Medical Assistance Percentage (FMAP) – which in turn could cause several states to roll back their Medicaid expansions and cause 20 million people to lose coverage. There are also proposals to limit Medicaid eligibility for immigrants. Medicaid currently pays for emergency medical services regardless of immigration status, of which most is for childbirth; and some states provide Medicaid coverage to undocumented children.
We’re concerned about the proposed spending cuts, and so is a significant part of the healthcare provider community. Medicaid is a program that covers 80 million people or 1 in 5 people living in the US, including children, pregnant people, and older adults in long-term care. These cuts would result in reduced access to not only clinical services, but also the many SDOH services that come through the Medicaid system.
In addition, protecting Medicaid coverage helps increase access to federal nutrition programs. The Medicaid system helps people access SNAP through outreach and care coordination services. Medicaid confers automatic eligibility for enrollees who fit WIC’s demographic requirements, and in fact, there is an explicit mandate that Medicaid coordinate with WIC.
Furthermore, Medicaid enrollment contributes to school meal utilization in likely-eligible communities. Forty three states have participated in a USDA demonstration project to directly certify students for free or reduced-price school meals using Medicaid data. In at least these 43 states, Medicaid enrollment data is part of the calculation to allow schools to adopt the Community Eligibility Provision (CEP). CEP is an option for communities to expand access to no-cost meals and reduce paperwork for schools and families by leveraging existing eligibility data about the number of children enrolled in other public benefits. In other words, maximizing Medicaid coverage means we achieve government efficiencies that maximize access to programs for eligible families and children.
However, it’s too soon to tell how these cuts might affect SDOH programming by state Medicaid systems. This is because state Medicaid programs may take different approaches to meet changing federal requirements and policies. In the meantime, we recommend following Families USA and its allies who are asking individuals to contact members of Congress to protect Medicaid.
Meanwhile, the reconciliation package passed by the House Budget Committee would direct the Agriculture committee to make $230 billion in cuts, most of which will probably come from SNAP. Such spending reduction would likely require limiting future revisions of the Thrifty Food Plan, the basis for SNAP benefit levels, if not an outright benefit cut or other major restructuring of the program. Other possibilities for SNAP cuts include eliminating Broad Based Categorical Eligibility (BBCE, an administrative streamlining option for states), imposing additional work-reporting requirements and participation time limits, capping maximum household size, and restricting adjustments to benefits based on inflation.
SNAP helps more than 41 million Americans afford groceries. Cutting benefits will make it harder for families to keep up with grocery prices and afford nutritious foods. The Center for Budget and Policy Priorities estimates that under this proposal, SNAP benefit amounts would shrink by around $42 per person per month, 9 million people would need to be removed from the program, or state governments would have to pick up the tab. Like for Medicaid, SNAP cuts will also create a ripple effect on other programs based on SNAP participation, like WIC (for which SNAP also confers automatic eligibility for women, infants, and children), and school meals via CEP – all while increasing administrative burden and cost.
Share Our Strength is calling on folks to contact their members of Congress to protect SNAP to support the food and nutrition security of children and their families.
Threats to immigrants
The threat of the Trump administration’s anti-immigrant policies will deter immigrant and mixed status families from accessing benefits despite their eligibility and the fact that immigrants pay taxes into the government systems that fund these benefits. WIC and emergency Medicaid are currently available to people who meet these program’s eligibility requirements, regardless of immigration status. Some states have gone further and expanded state-funded coverage to income-eligible people regardless of immigration status. SNAP is also available to some living in mixed status households, including US citizen children and those with a green card for at least 5 years (among limited types of non-citizens who can participate).
Immigration enforcement triggered by public benefit participation not only disrupts the health of families directly affected, but also causes hesitation to participate among other eligible immigrants. This “chilling effect” on SNAP and WIC participation already occurred when the federal government added these programs to the “Public Charge” Inadmissibility Rule in 2019. Even though this rule was short-lived and reversed in 2021, the changes generated fear and confusion, and a “chilling” effect which began in 2018 when the changes were proposed. This chilling effect resulted in reductions in SNAP and WIC participation and concerns among immigrant populations about participating in public benefits.
While we’re not sure whether the current Trump Administration will pursue the same public charge restrictions, their actions around deportation, passing an executive order to end birthright citizenship, DACA and rescinding a Biden-era policy that protected churches, schools, and hospitals from immigration enforcement may have similar effects on reducing use of public benefits and healthcare services among eligible immigrants. As of now, the Public Charge rule has not changed – follow the Protecting Immigrant Families coalition for up to date news and resources on this topic.
Food is Medicine as common ground – and where SNAP and WIC fit in
Newly confirmed Secretary of Health and Human Services Robert F. Kennedy Jr. has signalled a desire to end chronic disease and shake up the food system to prevent diet-related illnesses, an area of common interest for MFSN. RFK Jr.’s team and the Make America Healthy Again Congressional Caucus have named FIM as a key interest. The recently announced White House MAHA Commission calls out a need to improve child health, especially given the increasing prevalence of obesity, prediabetes, and fatty liver disease among young people. MFSN will be paying attention to how to engage this Commission in such a way that advances the food and nutrition security of children and families (without endorsing claims or policies that aren’t science-based).
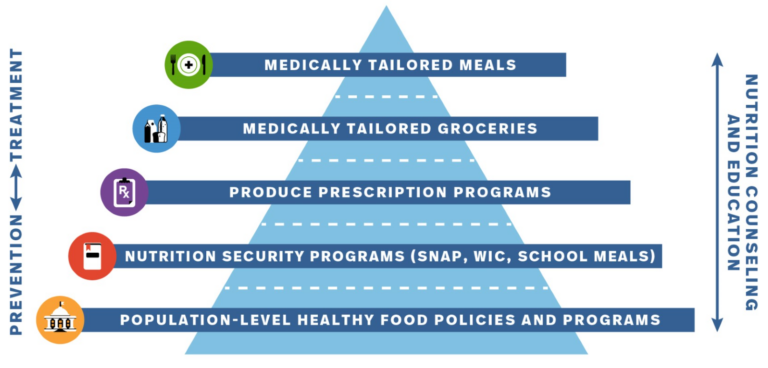
We see our position in MFSN as talking about how Food is Medicine as a continuum that includes federal nutrition benefits (SNAP, WIC, school meals, and Summer EBT). That continuum begins with disease prevention for people with food insecurity and extends into treatment for people with diet-related illnesses. At all stages of the prevention-to-treatment continuum, developing policies that strengthen SNAP and WIC, and healthcare-assisted application support for SNAP and WIC are important FIM strategies that complement medically tailored meals and groceries, and produce prescriptions.

Leaders in the field already conceptualize FIM as including federal nutrition benefits, particularly when a healthcare team assists with navigation support for patients/members with accessing SNAP and WIC. Moreover, there is strong evidence that SNAP is associated with healthcare savings ($1400 per Medicaid enrollee per year) and that WIC is associated with improved infant health outcomes – just to name a couple of the positive health outcomes related to these benefits.
In terms of the client experience, grocery provision, produce prescriptions, or meal provision interventions provide an environment for individuals and their families to eat healthier for free. Combined with nutrition education, this creates an enabling environment for developing healthier long-term diets. The final ingredient is having a healthcare team member or trusted community partner assist the patient with getting connected to SNAP and WIC. One real-life example is the Public Health Solutions Food Navigator Program – a partnership between Public Health Solutions, health systems like New York City Health + Hospitals, and other community organizations to assist food-insecure patients with access to SNAP, WIC, and food security programs. There are additive positive effects in bundled FIM approaches combining direct food provision, nutrition education, and benefits access. These policies and programs enable families to develop healthier dietary patterns that are more easily maintained even after direct food provision ends – thanks to the additional dollars in the pocket from federal nutrition benefits like SNAP and WIC.
Despite SNAP being a nutrition program, we do not support SNAP choice restriction as proposed by RFK Jr. and new USDA Secretary Brooke Rollins. Such policies would prevent participants from using SNAP to buy sugary beverages, processed foods, or anything else considered “unhealthy”. Despite the appeal of promoting healthy eating, MFSN is against SNAP choice restriction, and Gina Plata-Nino from FRAC lays out the argument best. In brief: preserving flexibility in what you can buy with SNAP enables families to make their own choices that meet their children’s health needs, lifestyle, and cultural preferences. SNAP choice restriction is also logistically challenging to implement because it means the private grocery sector needs to organize foods based on what is or isn’t allowed, which is both costly and could cause some grocery stores not to participate. Choice restriction also exacerbates stereotypes about SNAP participants, leading people to forego benefits they’re entitled to. Instead, nutrition education (such as through SNAP-Ed) and nutrition incentive programs like Double Bucks and produce prescriptions (which tend to give SNAP participants $40 or more per month extra to spend only on fruits and vegetables at grocery stores or farmers markets) increase healthy eating and preserve participant dignity, while also supporting local agriculture.
Nonetheless, we will continue talking about how SNAP is part of FIM, so that we can increase broader buy-in and protection of funding during this administration, and moreover, increase our collective opportunities to bundle services so that Medicaid participants can access comprehensive food and nutrition security services.
A possible path forward for food security in Medicaid
The previous Trump administration supported SDOH in Medicaid in some form. North Carolina implemented an 1115 Waiver with broad food and nutrition programming that the Trump administration CMS approved in 2017. CMS also released key guidance for covering SDOH services under Medicaid in January 2021 before the administration changed. In this letter to state Medicaid directors, CMS laid out a roadmap for addressing SDOH within Medicaid and CHIP. The guidance encouraged states to design programs around food security, housing, and other SDOH. CMS highlighted existing federal flexibilities and managed care tools – including 1115 waivers, In Lieu of Services, value-added services, quality measurement and improvement, and managed care contracting strategies. These are the tools we dive into in our MFSN Promising Strategies guidance paper.
SDOH investments within Medicaid can continue, especially when state governments drive these efforts, but the policy tools to achieve these goals will likely shift. 1115 Waivers to cover SDOH services proliferated under the Biden administration, but we expect 1115 Waivers may run into barriers because CMS plays a large role in negotiating and approving these waivers. Their approach to these negotiations will likely focus on cutting federal spending and encouraging states to add Medicaid work requirements. In fact, several states attempted to use 1115 waivers to establish work requirements during the first Trump administration. The Biden administration then rolled most of these back. These proposals have emerged or re-emerged in multiple states recently. We will continue to keep our eye on 1115 Waiver opportunities and will support their implementation in states that secured approvals from the outgoing Biden administration.
The upshot – 1115 waivers can take up to 5 years from advocating, planning, and designing to implementation. Therefore, it’s never too soon to start thinking about them and building coalitions of food security champions from the anti-hunger and healthcare communities. Such coalition-building is highly applicable and necessary to other forms of Medicaid policy advocacy and successful program implementation.
For this reason, MFSN is continuing to support state-based organizations working on Medicaid managed care opportunities to cover food and nutrition supports. Managed care organizations (MCOs) are the health insurance companies that in the majority of states, are the organizations through which a Medicaid enrollee gets their health insurance. Some examples of managed care opportunities:
- In Lieu of Services (ILOS) – which has been adopted in California and Michigan, and is under consideration in several other states. ILOS approval occurs through regional CMS offices with comparatively less federal negotiation and oversight. ILOS funding flexibility relies on the idea that its services would reduce healthcare costs, and program costs can be built into Medicaid “capitation rates” or the per-member cost that the state pays MCOs. Federal guidance has specifically endorsed the idea of using ILOS to pay for Food is Medicine programming, including linking people to SNAP and WIC. The Biden Administration built on the 2021 Trump Administration SDOH guidance by describing what types of SDOH services could be paid for through which Medicaid authorities, and there are overlaps as to what could be paid for through an 1115 waiver or ILOS.
- Medicaid managed care organization (MCO) procurement cycles are an opportunity to add requirements and incentives to work on food security. We’ve identified at least 16 states where MCOs are now subject to food security screening requirements for their Medicaid members (see our Policy Dashboard) – though implementation details and effectiveness are a whole area for near-future research. MCO procurement also includes the opportunities to require tools like Community Reinvestment, Performance Improvement Plans, and Value Added Services.
- Community Reinvestment: MCOs must devote a percentage of their profits to activities that improve community health. Medicaid contract re-procurement does not require federal-level legislation and less federal engagement than 1115 waivers (though CMS still approves MCO contracts).
- Performance Improvement Plans: Federal regulations require that MCOs must engage in activities to improve the quality of care. This includes requirements around drafting a quality strategy. One strategy for improving quality is focused Performance Improvement Plans where plans and their provider network will focus on improving performance on a specific metric. Some states are using Quality Improvement strategies to develop and improve activities around social needs.
- Value Added Services are voluntary services that MCOs can offer, which in many states takes the form of healthy food boxes or vouchers.
These Medicaid policy tools are not as highly visible as 1115 waivers and generally do not come with the same level of resources to expand HRSN service provision infrastructure. Nonetheless, managed care strategies offer transformative opportunities for Medicaid to contribute to food and nutrition security – both through mobilization of its health insurance and care provider workforces, and through dollars to be spent on food security services.
For a deep dive about these Medicaid managed care opportunities, check out the slides and recording from our January 30th MFSN virtual convening with a talk from RJ Briscione from HMA Associates, explore our MFSN Policy Dashboard to learn examples of these tools in action, and register for our first National Summit on May 7-8 in Washington DC where we’ll continue the dialogue about Medicaid food security strategies, and SNAP and WIC as part of Food is Medicine.