Subscribe to the MFSN News Digest.
Happy holidays, and thanks for being with us this year!
Despite cuts to federal programs and threats to our community members, we remain committed to supporting the food needs of children and families through increasing access to SNAP and WIC as part of the Food is Medicine (FIM) movement. As we reflect on this year, we’re proud to share highlights from what we accomplished together:
- Three virtual convenings plus our inaugural in-person MFSN Summit – read the Summit Report covering Medicaid policy changes, data sharing, equity and dignity, and research and evaluation for Food is Medicine (FIM) and food security strategies, as well as articulating our 2025-2026 strategies. We were proud to feature two speakers from the Share Our Strength SNAP Parent and Caregiver Advisory Council. Stories about how federal nutrition programs enabled healthier eating for their families are recapped in blog posts about Anthony Bonner and Ashleigh Ligon.
- Round 2 of the MFSN Partner Program with our 2026 grantees, while continuing to support our round 1 grantees and other partners as they continue advocating for Medicaid food security strategies. MFSN technical assistance contributed to key policy wins, including Oklahoma’s legislation to begin integrating the Medicaid, SNAP, and WIC applications, and Michigan’s nutrition In Lieu of Services program.
- Coalition-building by our grantees, including state FIM coalition launches in Ohio and New Mexico, and the inaugural Michigan Food as Medicine (MiFAM) Summit in October, organized by Food Bank Council of Michigan (FBCM), a 24-25 MFSN grantee. The MiFAM Summit brought together healthcare providers, community groups, policymakers, and researchers. Attendees described the Summit as “inspiring”, “energizing”, and “full of actionable strategies”. To continue the conversation and coalition-building, contact info@mifamsummit.org.
- Continued updates on the Medicaid Food Security Policy Dashboard: We review state Medicaid Managed Care Contracts, 1115 waivers, and other publicly available policy documents to compile a compendium of examples of how Medicaid addresses food insecurity among children and families. We were grateful to present the dashboard at the SIREN National Research Meeting.
- Our brief on the complementarity between healthcare-funded FIM and federally-funded SNAP and WIC nutrition benefits – written in partnership with the Center for Health Care Strategies (CHCS).
- Advocacy and engagement: Showing up at Capitol Hill in efforts led by the Tufts FIM Institute and National Produce Prescription Collaborative, being invited to great convenings like the Tufts FIM Summit and Aspen Institute Sharper Definitions of FIM event, and providing public comments on federal healthcare-food security policy issues.
Coming in early 2026: We’re working on a resource for policymakers and advocates about FIM cost-effectiveness analysis – be on the lookout for that in the coming weeks! We’re also working on developing other resources, research proposals, and our next round of MFSPP technical assistance grants – stay tuned for more announcements!
As we close out the year, we have two calls to action:
- Call on the government to maintain access to public benefits for immigrants. The Department of Homeland Security (DHS) announced a proposed “public charge” rule that will expand what counts against immigrant families when applying for green cards, putting parents in an impossible position of choosing between food and keeping their families together. DHS could count the use of any health or social service program, past or present, against them, including SNAP, WIC, and Medicaid, even when parents are participating in programs their families are eligible for under federal law. The proposal puts millions at risk because public charge restrictions have a chilling effect on immigrant public benefit participation. This means eligible families could then miss out on critical nutrition assistance and healthcare coverage. Please consider submitting a public comment by December 19 before DHS finalizes the rule. You can comment using this link with template language. See additional resources in the Protecting Immigrant Families coalition’s outreach toolkit.
- Ask Congress to reverse the nearly $200 billion in SNAP cuts. At the end of November, Senator Ben Ray Lujan (D-NM), Senate Agriculture Committee Ranking Member Amy Klobuchar (D-MN), Representative Jahana Hayes (D-CT), House Agriculture Committee Ranking Member Angie Craig (D-MN), with multiple cosponsors (in the Senate and House), introduced the Restoring Food Security for American Families and Farmers Act of 2025. This legislation would strike all harmful SNAP provisions from HR1, reversing the almost $200 billion in SNAP cuts. The timing of this bill sustains momentum for SNAP during the shutdown and underscores for Congress the devastating impact of SNAP cuts on families. We now call on members of Congress on both sides of the aisle to stand with families, farmers, and small businesses by passing this legislation. Tell Congress you support reversing SNAP cuts.
The year is winding down, but legislative and administrative changes affecting Medicaid and SNAP have not slowed. This digest provides Federal Policy Updates (including CMS guidance on Medicaid work requirements and updates on Rural Health Transformation Program applications), State Policy Updates (covering SNAP eligibility for immigrants, SNAP food restrictions, and Medicaid managed care updates), and Resources & Recommended Reading (focused on Medicaid food security strategies and FIM). Lastly, check out Upcoming Events and Opportunities.
Policy Highlights & Resources
Affordability most common barrier to healthy eating among people with food and nutrition insecurity
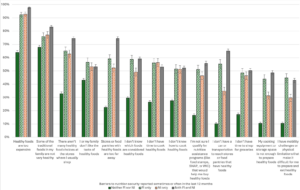
In the Tufts Food is Medicine Institute’s Nutrition Security Screener (NSS) study, researchers found that “Healthy foods are too expensive” was the top barrier to healthy eating, reported by over 90% of respondents with food insecurity, nutrition insecurity, or both. Other common barriers included traditional family foods not being healthy, and lack of healthy food access and/or choice. Barriers related to education were reported by about half of the sample. Half of food-insecure and nutrition-insecure respondents reported being unsure whether they qualify for nutrition assistance programs such as SNAP and WIC. This data reinforces MFSN’s call to address healthy food affordability through both healthcare-funded FIM and SNAP/WIC navigation assistance. Preliminary data from a Tufts study show that higher benefit amounts in produce prescriptions led to increases in voucher redemption and self-reported food security.
Both food insecurity (FI) and nutrition insecurity (NI) were predictive of chronic illnesses like diabetes, hypertension, high cholesterol, heart disease, and stroke. There was moderate overlap between people reporting food insecurity and nutrition insecurity, indicating a need for more insights on how and when to assess for FI and NI. In the NSS, patients or community members are asked how much difficulty they have with healthy eating and then prompted to choose from a list of barriers to healthy eating that they identify. Researchers tested the NSS among 20,523 adults in 5 diverse populations alongside FI screening using the previously validated Hunger Vital Sign and USDA six-item module. Dr. Dariush Mozaffarian presented findings from this paper at the Tufts FIM Summit in October (slides and recording of his talk here).
Federal Policy Updates
Nutrition supports in the 2026 Medicare Physician Fee Schedule final rule
CMS released the 2026 Medicare Physician Fee Schedule final rule, which sets Medicare policy and influences healthcare system approaches to Medicaid. Despite advocacy led by our partners at FMIC about adding a separate billing pathway for medically tailored meals (MTM), CMS ultimately did not include it, saying, “We acknowledge commenters’ feedback regarding the addition of medically tailored meal benefits to MDPP…MDPP suppliers have the flexibility to provide Beneficiary Engagement Incentives (BEIs) to support program goals. Since medically tailored meals are considered a BEI, we are not revising the MDPP payment methodology to separately account for medically tailored meals at this time.”
The 2026 rule also touches on HRSN service provision. CMS revised billing code G0136, which in 2024 was defined as “Administration of a standardized, evidence-based social determinants of health risk assessment tool, 5 to 15 minutes, not more often than every 6 months”. CMS proposed deleting this code, but, in response to comments, decided to retitle and narrow it to: “Administration of a standardized, evidence-based assessment of physical activity and nutrition, 5-15 minutes, not more often than every 6 months”. The rule names several dietary quality assessments, such as Mini-EAT, STC, and others.
The rule continues an emphasis on HRSN screening and intervention. CMS revised the Community Health Integration code G0019 to refer to activities addressing “upstream drivers of health” instead of SDOH. The rule explains, “The term ‘upstream driver(s)’ encompasses a wider range of root causes of the problems that practitioners are addressing through CHI services. This type of whole-person care can better address the upstream drivers that affect patient behaviors (such as smoking, poor nutrition, low physical activity, substance misuse, etc.) or potential dietary, behavioral, medical, and environmental drivers to lessen the impacts of the problem(s) addressed in the initiating visit.” In addition, the 2026 Rule includes a section on increasing HRSN screening uptake among patients in the new Ambulatory Specialty Model, aimed at improving care for heart failure and low back pain.
Food and nutrition features heavily in state applications for Rural Health Transformation Program
All 50 states have applied for the $50B Rural Health Transformation Program created by HR1, according to CMS. Food and nutrition were a common theme within states’ RHTP applications. State Health and Value Strategies has posted a tracker of state RHTP applications and an initial theme analysis. Stateline also conducted an analysis of 10 state proposals.
Share Our Strength submitted a comment, based on our experience leading the Healthy Families Rx program, that influenced Louisiana’s application and its inclusion of “food FARMacy” programs. MFSN also supported grantees with comment submissions that led to their states mentioning food security, nutrition education, and/or FIM as priorities in Georgia, Virginia, and Texas.
CMS Issues New State Guidance on Medicaid Work Requirements
The Centers for Medicare & Medicaid Services (CMS) has provided guidance on implementing work requirements under HR1’s new community engagement provision. According to CMS, work reforms will be based on four principles: connect members to work and community, state flexibility, promote alignment, and protect taxpayers. CMS claims this guidance will help align Medicaid with other public benefits such as SNAP and Temporary Assistance for Needy Families (TANF). States must implement these requirements by January 1, 2027. The KFF Medicaid survey identified state agencies’ anticipated barriers to implementing Medicaid work requirements.
House Democrats Introduce Legislation to Restore USDA’s Annual Food Security Access Report
US Representatives Wesley Bill and Nanette Barragán introduced the Food Assurance and Security Act to restore the Household Food Security Report, which the USDA cancelled earlier this year. Crystal FitzSimons, president of FRAC, is quoted, “This report has been our roadmap to understanding who is struggling to put food on the table, and the solutions needed to ensure no one goes hungry in the world’s wealthiest nation. ”
A View of Medicaid from a Recent Annual Medicaid Budget Survey
As states completed the unwinding of pandemic-era continuous coverage, KFF’s 2025-2026 Medicaid Budget Survey found that Medicaid enrollment fell 7.6% in FY2025 and is expected to be flat in FY2026. Total Medicaid spending grew by 8.6% in FY2025 and is expected to grow by 7.9% in FY2026. A KFF brief discusses how Medicaid unwinding reduced total enrollment, but factors such as states’ continuous eligibility provisions for children and postpartum individuals also drove enrollment. Drivers of Medicaid spending growth included MCO rate increases, higher healthcare needs among enrollees post-unwinding, and increasing long-term care, pharmacy, and behavioral health care costs.
Sixteen state Medicaid programs reported covering GLP-1s for obesity treatment, and some states plan to restrict coverage due to their significant contribution to healthcare cost growth. For example, New Hampshire and Pennsylvania have decided to end Medicaid coverage of GLP-1 medications used solely for weight loss beginning January 1. GLP-1s are statutorily required to be covered for their original indications for diabetes and other chronic illnesses, but obesity treatment coverage is optional. The Tufts Food is Medicine Institute has written about how FIM and nutrition support, including MTM, MTG, PRx, and nutrition benefit navigation assistance, could help improve outcomes and reduce costs relating to GLP-1 use.
GAO raises concerns about how CMS is determining 1115 waiver budget neutrality
The Government Accountability Office recommended that CMS should “stop treating costs for populations or services that could not have otherwise been covered under existing Medicaid authorities as hypothetical when setting demonstration spending limits. Instead, CMS should require the costs of those populations or services to be offset by other reductions in demonstration spending.” Relatedly, HR1 now requires the CMS Chief Actuary to certify state 1115 waivers for budget neutrality rather than the HHS Secretary. Even though budget neutrality was already required in 1115 waivers, the HR1 provision and GAO report suggest the federal government will be looking more closely at cost control and/or cost-effectiveness.
State Policy Updates
USDA updates guidance after 21 states and DC sue over changes to immigrants’ SNAP eligibility
USDA clarified in its December 9 guidance to SNAP state agencies that lawful permanent residents (LPRs) who entered as, or were granted, humanitarian immigrant status are eligible for SNAP without a five-year waiting period. This guidance was issued after attorneys general from 21 states and DC filed a lawsuit alleging that USDA guidance incorrectly asserted that some lawful permanent residents are ineligible for SNAP. The lawsuit asked a federal court to bar the USDA from implementing the guidance. In response, the USDA had threatened to withhold funds from these states.
More states add SNAP choice restrictions in 2026
Hawaii, Missouri, North Dakota, South Carolina, Tennessee, and Virginia will now ban the use of SNAP benefits to buy soda, energy drinks, candy, and processed foods. The USDA has approved waivers for 18 states to restrict SNAP food purchases as early as January 1. As FRAC has written about, these policies could create more risks than benefits for participants and food businesses.
Idaho Medicaid seeks public input on transition to comprehensive managed care
Idaho is transitioning to a Medicaid managed care system where the state contracts with managed care organizations (MCOs) to coordinate and deliver Medicaid services. The Medicaid agency is requesting public feedback to shape the managed care transition. As MFSN has discussed, MCO contracting is an opportunity to add requirements for Medicaid food security strategies. The public input deadline is December 31.
Louisiana terminates UnitedHealthcare’s Medicaid MCO Contract
Louisiana’s Department of Health (LDH) will end its Medicaid contract with MCO UnitedHealthcare of Louisiana, effective January 1, after initially renewing all six MCO contracts through 2026. The state cited litigation involving pharmacy benefit managers linked to UnitedHealthcare and CVS Health/Aetna for the decision. However, after discussions, the state reversed its decision to cancel Aetna’s contract. UnitedHealthcare’s 330,700 Medicaid members must transition to one of the remaining MCOs: Aetna, AmeriHealth Caritas, Elevance Health, Humana, or Centene/Louisiana Healthcare Connections.
Colorado Governor proposes Medicaid cost cuts
Governor Jared Polis’s recommended FY2027 budget proposes significant Medicaid cost reductions, including limiting home caregiver hours, capping specific reimbursement rates, and restricting dental benefits. The $300 million increase in Medicaid spending is less than half of what is required to maintain the program’s current services. At the same time, Colorado plans to launch its 1115 waiver nutrition supports—counseling, groceries, and medically tailored meals for at-risk individuals, children, and pregnant individuals—in July 2027, financed by savings from the initial 1115 housing services rollout, which began in July of this year.
Resources & Recommended Reading
SNAP post-government shutdown
The government shutdown created a food crisis for millions of families, and although SNAP benefits have resumed, experts remain concerned about long-term economic damage to households with low incomes. It also revived questions about the 50-year-old SNAP formula, which advocates say does not keep up with the actual costs of healthy eating.
Millions will soon lose SNAP benefits under HR1. Not only does the bill create additional work requirements for SNAP participants, but it also shifts billions of dollars in costs to states, creating a potential financial crisis for 26 states due to their own tax cuts.
In some states, federal policy changes have highlighted the need for a streamlined process that includes modernizing benefits access systems, adding SNAP navigation assistance, or implementing other administrative changes. States are building integrated eligibility and enrollment (IEE) systems for core public benefit programs, including SNAP and Medicaid. These systems have the potential to help reduce the paperwork burdens that are estimated to cost 1 in 8 working-age SNAP participants their benefits. Economists found that scheduling flexibility for mandatory application interviews in California reduced credit card delinquency among participants.
Food is Medicine (FIM)
Politico article covers NC Medicaid 1115 waiver’s demonstrated savings and termination
This article examines North Carolina’s Healthy Opportunities Pilot and its 1115 waiver, which provided food and other HRSN support. Despite demonstrated savings and benefits for participants and rural economies, the state legislature opted not to fund the HOP program’s statewide expansion. NC leaders and advocates have noted that this decision was driven by NC-specific nuances around political context and branding around their 1115 waiver, and therefore, that advocates in other states could learn from NC while still continuing to work on Medicaid food security strategies. See our November Quarterly Convening recording, where participants from NC discuss this. Note that the Politico article does not mention how the 2021 SDOH guidance and 2023 ILOS guidance remain in place, and that despite rescission of the 2024 HRSN guidance, CMS is still reviewing 1115 waivers on a case-by-case basis, such as for Maine, which remains under consideration.
NY State efforts in Food Is Medicine under the 1115 waiver
New York’s 1115 waiver enables providers to screen patients for food insecurity and connect them to Medicaid-covered nutrition supports. The Regional Food Bank of Northeastern New York’s “Food Farmacy” program is showing how regular deliveries of healthy foods paired with nutrition counseling can improve outcomes for patients with diet-related conditions. Meanwhile, medically-tailored meal organization God’s Love We Deliver (GLWD) has added a screening tool on its website that lets individuals check whether they qualify for MTM or MTG. Under the 1115 waiver, GLWD expanded a team of community health workers to help individuals navigate social assistance programs in addition to their direct food provision services. The CHWs conduct eligibility screening for assistance programs and other 1115 waiver HRSN services, then refer clients using a closed-loop referral system.
Blue Cross NC randomized trial shows healthy food subsidy slightly more effective than food box
A UNC Health and Blue Cross NC clinical trial found that monthly grocery cards lowered blood pressure more effectively than delivering pre-selected healthy food boxes. Nonetheless, both approaches reduced food insecurity and improved blood pressure. The study provides clinical evidence on how increasing healthy food affordability and access can better support chronic disease management.
Grocery program shows improved healthcare engagement, but not improved diabetes control
This randomized trial tested whether giving people with diabetes and food insecurity healthy groceries plus dietitian support, coaching, and education would improve blood sugar control. For study participants, the FIM program increased preventive health engagement but was not associated with improved glycemic control. The study was limited by being conducted during the COVID-19 pandemic at only one health system with high-quality diabetes care for the control group (thereby reducing the measurable improvement due to FIM) and by a relatively short evaluation period.
Pear Suite and Instacart Partner to Increase Access to Food Resources for Medicaid Populations
Pear Suite and Instacart have launched a partnership to bring FIM services to Medicaid members nationwide, combining Pear Suite’s digital platform for community-health workers with Instacart’s grocery delivery and Fresh Funds stipends to help address food insecurity. Instacart also recently published an updated Health Policy Agenda highlighting its food access and FIM priorities.
MAHA’s Low-Hanging Fruit: Enabling Health Systems to Deploy Food as Medicine
The article spotlights how fraud-and-abuse regulations undermine federal priorities for chronic-disease prevention by discouraging providers from offering non-medical supports like nutritious food, transportation, and home-modification assistance. Although a HHS OIG recent advisory opinion gives one health center limited flexibility to offer such services, it also underscores that providers still face legal uncertainty and administrative burden when trying to address patients’ basic health-enabling needs. Without clearer protections, health systems will remain constrained from investing in upstream interventions that could lower costs, improve outcomes, and advance value-based care.
Medicaid
Center on Budget and Policy Priorities (CBPP) releases toolkit on Medicaid work requirements
CBPP explains how Medicaid’s new HR1 work requirements, starting in 2027, could cause many eligible people to lose coverage due to complex reporting and documentation rules. The toolkit outlines policy and implementation choices states can use to reduce red tape and keep eligible enrollees covered. It highlights that coordinating Medicaid with SNAP, such as using SNAP eligibility and verification data to identify exemptions and streamline renewals, is one of the most effective tools to prevent unnecessary coverage losses. These steps can help states protect access to care while meeting federal implementation requirements.
Medicaid Beneficiary Advisory Councils: A Guide to Evaluating Process and Impact (CHCS)
A CMS rule requires states to establish Beneficiary Advisory Councils (BACs) composed of Medicaid members, families, and caregivers, to inform policy development. A newly released toolkit, created by the Centers for Health Care Strategies (CHCS), offers strategies and examples for integrating evaluation into BAC programs. States can utilize evaluation to monitor progress, demonstrate impact, and improve BAC functionality and member experience.
Value-Based Payments Associated With Improved Quality Of Care at FQHCs
A Health Affairs study finds that although value-based payment (VBP) participation among federally qualified health centers (FQHCs) remains limited, even modest involvement is linked to improvements across multiple preventive and primary care quality measures. The findings highlight both the promise of VBP models to strengthen care in the safety net and the barriers FQHCs still face in adopting them at scale. The MFSN Policy Dashboard offers examples of value-based payments that integrate health-related social needs (HRSN).
Children’s Health
Children’s Medicaid Enrollment Increased after 12-month continuous coverage requirement
The Consolidated Appropriations Act of 2023 established a requirement to keep children enrolled in Medicaid for 12 months. This change led to higher children’s Medicaid enrollment. This is important for food security because Medicaid confers automatic eligibility for WIC (for pregnant individuals and children under 5) and contributes to school meal access due to the Community Eligibility Provision and Medicaid-direct-certification programs. CMS has stated it will no longer approve 1115 waivers to extend the child coverage window to 24 months or beyond, as several states have already done
Universal school meals associated with better blood pressure outcomes in children
A JAMA study found that universal free school meals policies, such as the Community Eligibility Provision, are linked to lower childhood blood pressure. The researchers suggest that improved access to nutritious school meals may help reduce early risk factors for cardiovascular disease, highlighting universal meals as a promising population-level strategy to support children’s long-term health.
Upcoming Events & Opportunities
December 17: Join the National Alliance for Impacting the Social Determinants of Health’s (NASDOH) webinar, “Policy Landscape of Upstream Drivers of Health,” for a discussion on the evolving federal policy landscape, including the latest changes to Medicaid. Register here.
December 17: Members of the National Produce Prescription Collaborative (NPPC) will join together for the NPPC’s annual virtual meeting at 12:30 pm ET. Member organizations can register here.
January 15: HealthBegins’ Kathryn Jantz will speak at the 2026 Colorado Food is Medicine Summit, 8 am – 4:30 pm MT. FIM leaders, practitioners, and advocates will gather to share and collaborate on innovative research and programs that will build sustainable solutions. Register here.
January 28: Join the INSPIRE Community Engagement Learning Network at 3 pm ET for a monthly series where professionals working on community engagement and people with lived experience connect and learn together. Register here for one or more meetings in the series.
January 30: Applications from state Medicaid agencies are being requested for the 2026 Center for Maternal & Child Health Medicaid Partnerships (CMMP) State TA. This HRSA-funded partnership between Altarum, the Association of Maternal Child Health Programs (AMCHP), and the Center for Health Care Strategies (CHCS) supports states/territories in aligning their Title V, Medicaid, and Children’s Health Insurance Program (CHIP) programs to improve maternal and child health outcomes.
Questions? Story Ideas?
- Contact: MFSN@strength.org
- Subscribe to our News Digest. To submit content for consideration, please email MFSN@strength.org with shareable language and links to content.